Problem Severity
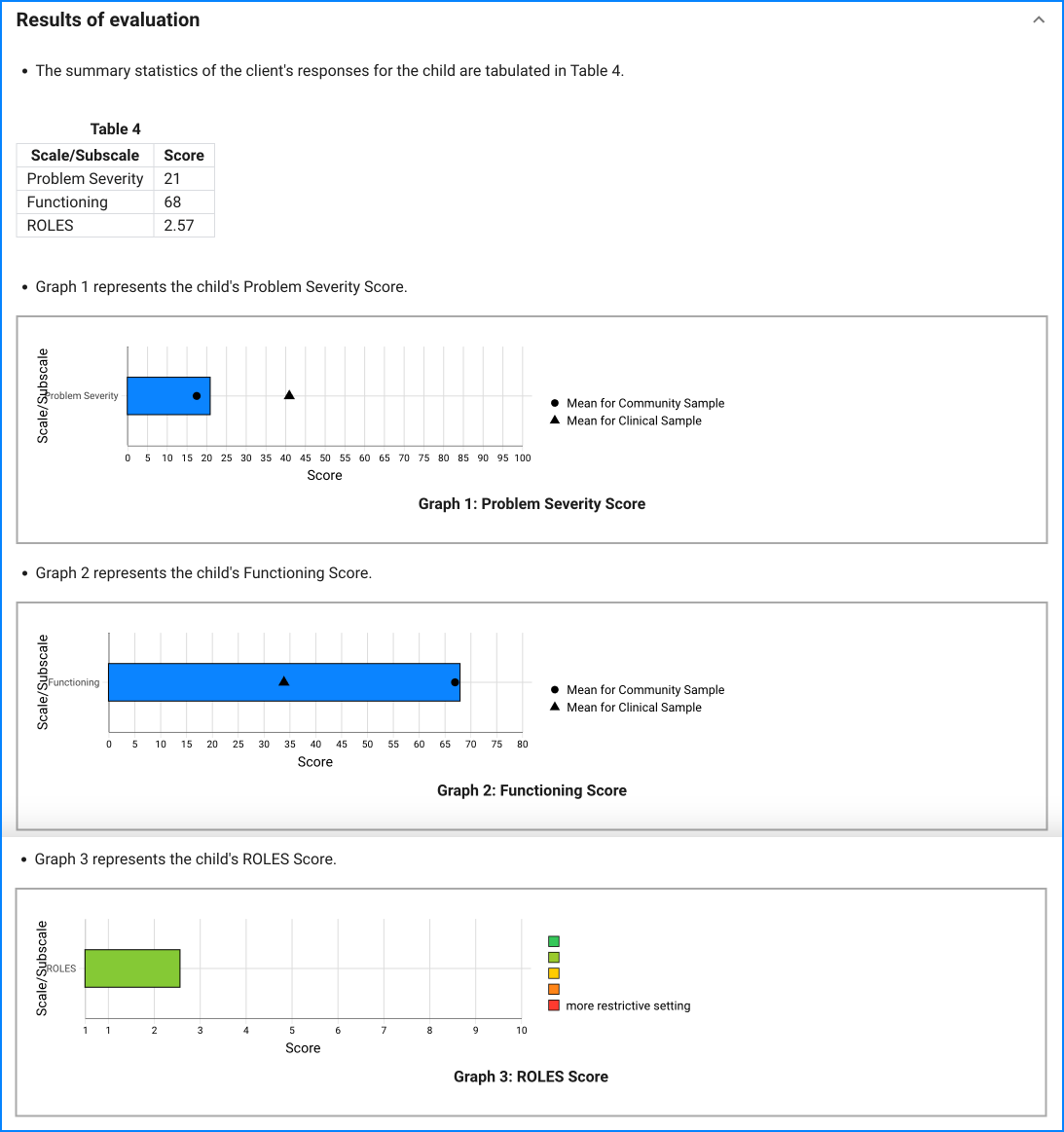
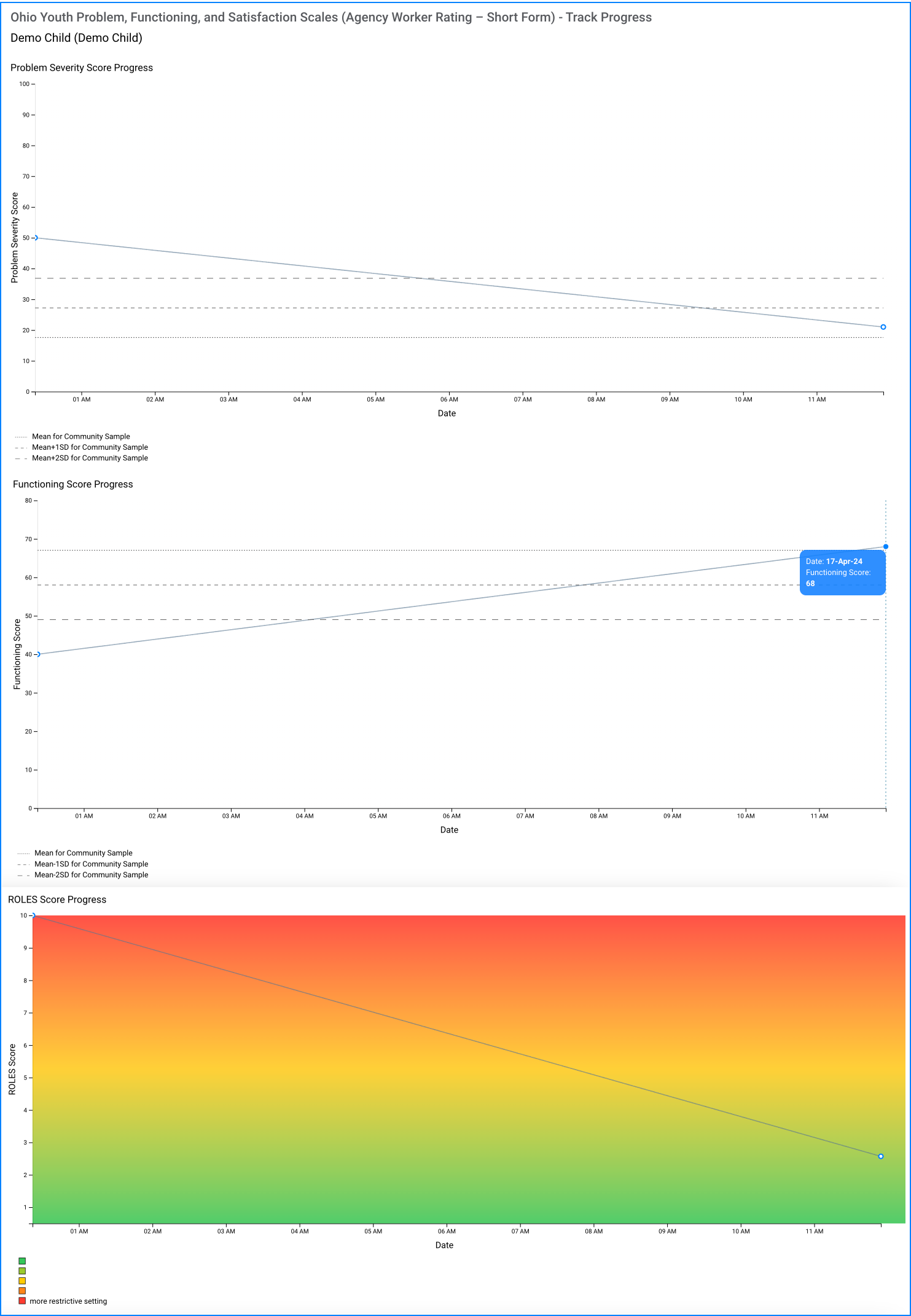
All three forms include the 20 item problem severity scale. Each of these items is rated on a 6-point scale for frequency during the past 30 days: not at all, once or twice, several times, often, most of the time, or all of the time. The columns for each frequency are coded respectively from 0 (Not at all) to 5 (All of the Time). Each column's score can then easily be added at the bottom of the page. The sum of the six columns then becomes the individual's score on the problem severity scale. No items are reverse-scored.
Functioning
The functioning scale total is calculated in the same manner used on the problem severity scale. Each of the 20 items is rated on its 5-point scale. The rating for each item is circled. The columns for each frequency are coded respectively from 0 (extreme troubles) to 4 (doing very well). Each column's score can then easily be added at the bottom of the page. The sum of the five columns then becomes the individual's score on the functioning scale. No items are reverse scored.
Restrictiveness of Living Environments Scale (ROLES)
The W-form includes a copy of the ROLES (Hawkins et al., 1986). The ROLES consists of a list of 23 categories of residential settings. Next to each specific setting is a blank line on which the agency worker writes the number of days (during the past 90 days) the youth was residing in that setting (The total of all the days will therefore add to 90).
Each setting is given a statistical 'weight' as listed in below. To get the ROLES total score, each weight is multiplied by the number of days in the blank next to the setting. The sum of these products is then calculated to get a total. The total is then divided by 90 to get the average restrictiveness for the previous 90 days.
Jail 10.0
Juvenile Detention Center 9.0
Inpatient Psychiatric Hospital 8.5
Drug/Alcohol Rehabilitation Center 8.0
Medical Hospital 7.5
Residential Treatment 6.5
Group Emergency Shelter 6.0
Residential Job Corp/Vocational Center 5.5
Group Home 5.5
Therapeutic Foster Care 5.0
Individual Home Emergency Shelter 5.0
Specialized Foster Care 4.5
Foster Care 4.0
Supervised Independent Living 3.5
Home of a Family Friend 2.5
Adoptive Home 2.5
Home of a Relative 2.5
School Dormitory 2.0
Biological Father 2.0
Biological Mother 2.0
Two Biological Parents 2.0
Independent Living with Friend 1.5
Independent Living by Self 0.5